
Does Your Organization Follow Best Practices for Documentation?
Documentation deficiencies lead to settled claim
A 32-year-old woman was admitted by her family physician (FP) to the hospital for induction of labor at 41 weeks, 4 days. She had a detailed birth plan including the use of a birthing ball. The FP ordered intermittent electronic fetal monitoring (EFM) during labor to allow the use of the birthing ball.
The labor and delivery (L & D) nurses’ efforts to monitor the fetal heart rate (FHR) were hampered by the woman’s firm insistence on adherence to her birth plan and the use of the birthing ball. Nursing notes were made every 30 minutes; however, key discussions with the mother were not included in the documentation and therefore not communicated to the FP. The woman refused most monitoring attempts despite explanations of the rationale for monitoring the baby’s FHR during rapidly progressing labor.
After birth, the baby was diagnosed with hypoxic ischemic encephalopathy, spastic quadriplegia and cerebral palsy. Years later the woman filed a malpractice claim alleging a delay in recognition and treatment of fetal distress resulting in permanent neurological injury. Due to the documentation deficiencies, especially the lack of documentation of her refusal to be monitored, and the team communication breakdowns, the claim was difficult to defend. The claim was settled with a payment made to the woman on behalf of the hospital and the FP.
Documentation not only serves as a defense against allegations of malpractice but is also the primary mechanism for communication among clinicians and care teams.
Malpractice claims with documentation deficiencies
An analysis of Constellation malpractice claims reveals that communication breakdowns occur in 35% of claims and represent 38% of costs. Documentation deficiencies contribute to 15% of claims and account for 22% of costs.
Top allegations with documentation deficiencies
The top allegations with documentation deficiencies as a contributing factor in harm events are:
- Surgical treatment
- Medical treatment
- Diagnosis-related
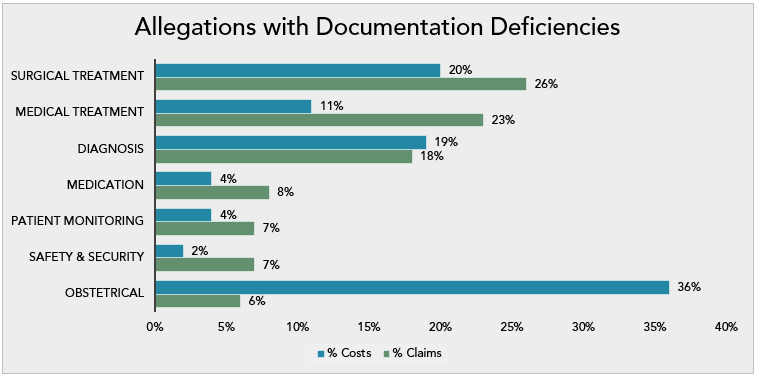
Of note are the obstetrical (OB) claims with documentation deficiencies, they account for 36% of costs while representing only 6% of claims.
A deeper analysis of all claims with documentation deficiencies reveals that when refusal of treatment is an issue, claims with insufficient documentation close with an average payment of over $2 million.
In their 2020 National CBS Report, The Power to Predict, CRICO Strategies’ research shows that the odds of a malpractice claim closing with a payment increase by 76% when there is insufficient documentation. Claims that had absent or insufficient documentation closed with payment 56% of the time compared to 30% for all cases, and 5% of these claims closed for $1 million+ compared to 4% for all claims.
Locations and teams responsible for care
The top locations and clinical teams involved in documentation claims are:
- Emergency department (ED) – 9% claims; 21% costs
- Labor and delivery (L & D) – 5% claims; 20% costs
- Clinic – 27% claims; 15% costs
- Patient hospital room – 18% claims; 13% of costs
- Hospital operating room –12% claims; 8% costs

Claims arising from care provided in the Emergency Department (ED) and L & D account for only 14% of claims with documentation deficiencies, but almost half (41%) of costs.
The majority (70%) of L & D claims with documentation deficiencies resulted in high severity injuries such as permanent neurologic injury. ED claims with documentation deficiencies resulted in high severity injuries, including death, in half (50%) of claims.
Best practices for quality documentation
For the best practices for quality documentation, simply remember the FACTS:
- Factual – specific, objective, respectful, descriptive
- Accurate – precise, descriptive, measurable, mutually-understood
- Complete – thorough, chronologic, clear, includes communications
- Timely – prompt, immediate, can include appropriate late entry/addendums
- Special situations – distinguished by some unusual characteristics
“Documentation using FACTS can help facilitate appropriate medical decision-making based on a more factual, accurate, complete and timely entry.”
Karie Minaga-Miya, Senior Risk Consultant at Constellation
How to improve documentation in your organization
- Assemble a diverse work group to:
- Study the current documentation system and identify ways to improve
- Develop and implement policies that guide clinicians and care team members with documentation expectations
- Educate clinicians and care team members on your documentation standards using actual documentation deficiency case examples
- Periodically audit medical records for adherence to standards
- Engage care team members to coach peers when they see nonadherence with documentation standards
- Encourage care team members to report barriers to meeting documentation standards
The HEAL Prepare Toolkit
Our HEAL Prepare Toolkit helps your organization prepare and respond to harm events. Unit 2, Event Response, can help you understand how contributing factors, like documentation deficiencies, can disrupt communication among the team, affect clinician decision-making leading to harm and cause difficulties defending allegations of malpractice.
Start your journey by taking the HEAL Assessment and then the Action Plan will guide you through the Toolkit’s four units: (1) culture, (2) event response, (3) patient communication, and (4) moving forward. Sign in to ConstellationMutual.com to access the HEAL Prepare Toolkit found in Risk Resources.
Constellation’s HEAL program provides healing benefits for care teams and their organizations because we truly believe that what’s good for care teams is good for business.
Constellation and HEAL are trademarks of Constellation, Inc.
Share this blog article:
Latest Blog Articles
Five Steps to Reduce Generative AI Risks in Healthcare
AI is already assisting physicians and healthcare organizations in many ways. Learn how its use may impact liability and what strategies can mitigate risk.
Five Steps to Reduce Obstetrical Errors and Malpractice Claims
Learn how to reduce obstetrical harm using evidence-based protocols for managing high-risk situations, joint team fetal monitoring education, and enhanced teamwork.
How to Reduce Surgical Harm and Malpractice Claims
In an analysis of our medical professional liability claims, surgical allegations are #1 in occurrence and #2 in cost. Learn how to reduce surgical malpractice risk.