
Five Ways to Mitigate Obstetrical-Related Harm
Delay in recognition and treatment of fetal distress results in significant injuries to a baby
A 22-year-old pregnant woman was admitted to the hospital in the middle of the night in active labor at 39 weeks gestation. This was her first pregnancy. The obstetrician (OB) ruptured the woman’s membranes and ordered electronic fetal monitoring (EFM), which showed a reassuring category I fetal heart rate (FHR) pattern throughout the rest of the night.

At 3:00 p.m. after pushing for several hours, the woman’s labor and delivery (L & D) nurse noted a category II FHR pattern and administered oxygen. At 3:53 and 4:06 p.m., the L & D nurse contacted the OB about her concerns for fetal wellbeing. The OB arrived at the hospital at 4:15 p.m., reviewed the EFM strips, and noted the FHR was 200 beats per minute (BPM) with absent variability. The OB encountered difficulty with attempts of vaginal delivery and used a vacuum and forceps to deliver the baby at 4:40 p.m. The baby was born with a nuchal cord and no respiratory effort. The team intubated the baby and admitted her to the NICU with active seizures. The baby girl was diagnosed with significant neurological injuries and showed developmental delays in the years following before her death at five years of age.
The parents filed a malpractice claim against the OB and the hospital (L & D nurses), alleging delay in recognition and treatment of fetal distress, failure to recognize cephalopelvic disproportion (CPD), and failure to perform a cesarean section (C-section) in a timely manner. The experts who reviewed the case were critical of the L & D nursing team for failing to recognize troublesome FHR patterns early in the morning after admission, especially after pushing began, and then failing to communicate the situation to the OB. During the claim investigation, it was noted that there were discrepancies in the nursing notes and the OB’s memory about what information was communicated about the progress of labor and fetal status. The experts were critical of the OB for failing to recognize CPD and an abnormal labor curve and for failing to perform an emergency C-section. The case was closed with a payment made to the parents on behalf of the OB and the hospital.
Top allegations in obstetrical malpractice claims
An analysis of our malpractice claims reveals that obstetrical claims are third in total cost—despite representing only 4% of claims—and have the highest average settlement payments when care issues are present.
Delay in recognition and treatment of fetal distress is the top OB allegation in both percent of claims and cost.
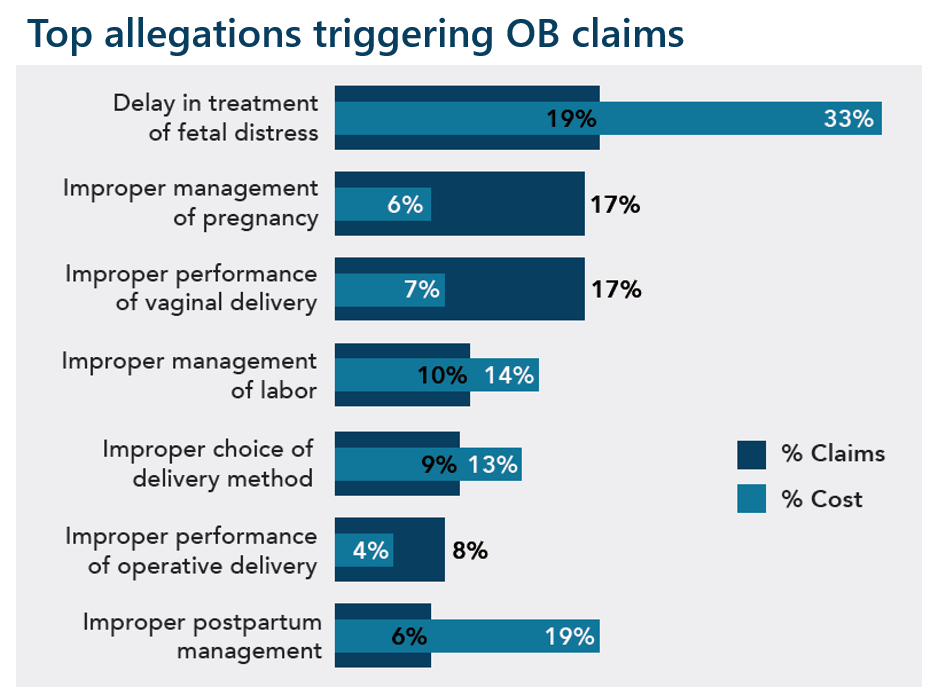
All graphs represent malpractice claims reviewed as of 12/31/2020
Top contributing factors involved in OB claims
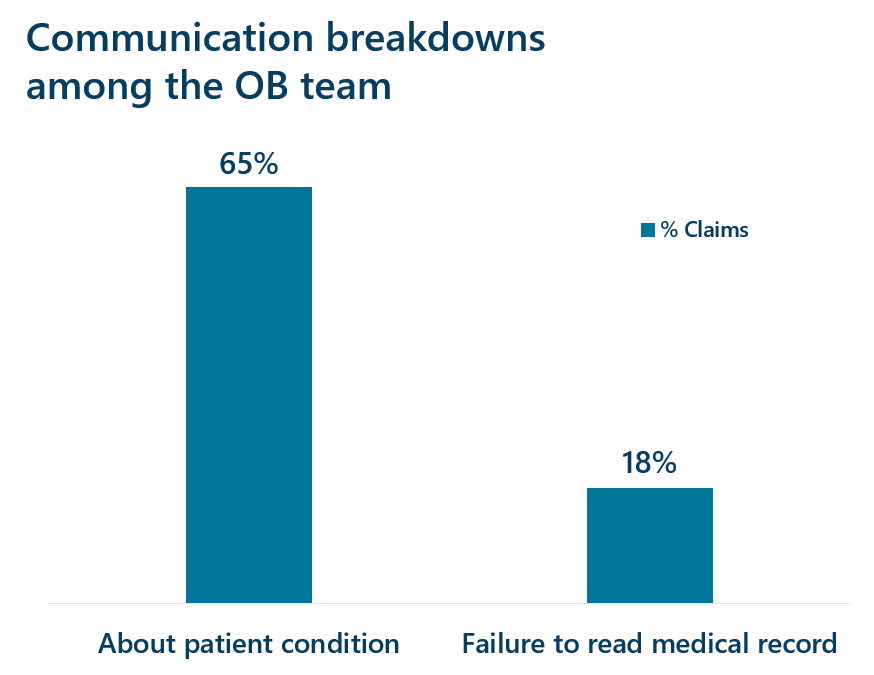
Several of the top contributing factors involved in obstetrical claims include patient assessment issues, communication breakdowns among the OB team, and a delay in recognition and treatment of fetal distress. In 44% of OB claims, a secondary responsible clinician was named; over half of these claims involved nursing and allegations of delay in recognition and treatment of fetal distress. These findings highlight potential gaps in fetal monitoring and team communication skills, as the case above illustrates.
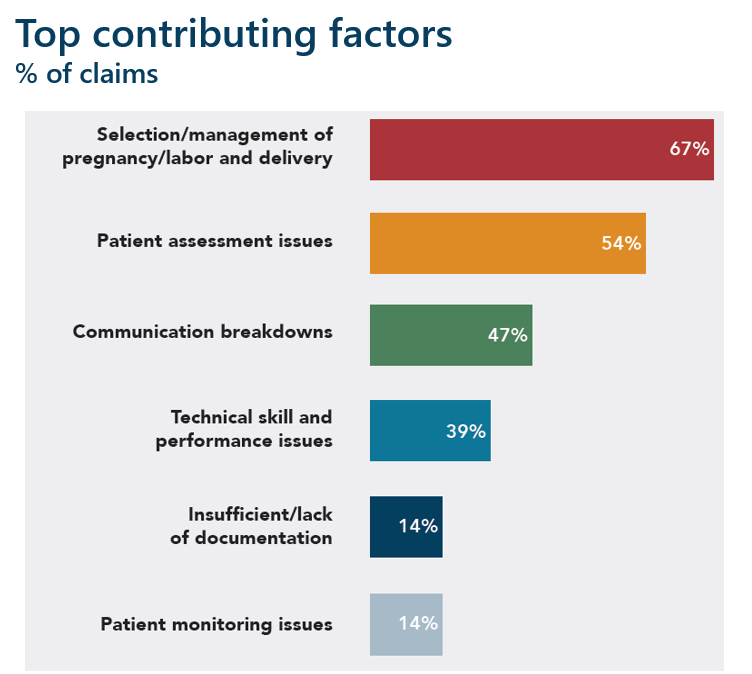
These factors contribute to harm/malpractice claims and are amenable to risk mitigation strategies. A single harm event may involve multiple contributing factors.
Five ways to mitigate OB-related harm and malpractice claims
- Provide joint clinician and nursing team training and education using a comprehensive, evidence-based electronic FHR monitoring education program such as Relias Obstetrics Solution. Ensure all team members who review and assess electronic FHR monitor tracings are certified in electronic fetal monitoring.
- Perform multi-disciplinary drills and simulations on low-frequency, high-severity events (e.g., non-reassuring fetal heart rate, shoulder dystocia, OB hemorrhage, prolapsed umbilical cord, and placental abruption).
- Invest in team training and communication skills using tools such as SBAR and I-PASS.
- Use OB documentation templates embedded in the electronic health record to help with complete and accurate documentation of events.
- To guide practice, implement evidence-based safety bundles, such as the AIM Patient Safety Bundles. These bundles are a structured way of improving the processes of care and patient outcomes.
Watch the webinar rewind, Reducing Obstetrical Harm With Electronic Fetal Monitoring Team Training, to learn more about mitigating obstetrical-related harm.
*Follow: MyAccount > Risk Resources > Bundled Solutions > Obstetrics
Share this blog article:
Latest Blog Articles
Five Steps to Reduce Generative AI Risks in Healthcare
AI is already assisting physicians and healthcare organizations in many ways. Learn how its use may impact liability and what strategies can mitigate risk.
Five Steps to Reduce Obstetrical Errors and Malpractice Claims
Learn how to reduce obstetrical harm using evidence-based protocols for managing high-risk situations, joint team fetal monitoring education, and enhanced teamwork.
How to Reduce Surgical Harm and Malpractice Claims
In an analysis of our medical professional liability claims, surgical allegations are #1 in occurrence and #2 in cost. Learn how to reduce surgical malpractice risk.