
Who Is Most at Risk for Diagnostic Error Malpractice Claims?
Failure to timely diagnose subarachnoid hemorrhage in the ED results in death
A 60-year-old woman presented to the emergency department (ED) of her local hospital with complaints of sudden onset neck pain that began four days earlier and radiated up to her head. She described the pain as so severe that it made her nauseated, and turning her head from side to side worsened the pain and caused dizziness. She denied any trauma.

The ED physician examined the woman and documented that her neck was tender to palpitation, and she had pain when turning her head from side to side. He documented his diagnosis as a neck muscle spasm, prescribed Tramadol, and instructed her to continue taking ibuprofen and use a heating pad as needed. He did not document a neurologic exam.
The next day, she presented to another ED with complaints of continued neck pain, headache, and an inability to move her neck without pain. She described her headache as “not the worst ever” but described the neck pain as “the worst ever.” An ED physician assistant performed a physical exam and noted obvious neck pain, bilateral muscle spasms, and that she could not flex or extend her neck. He ordered a head CT without contrast, which was interpreted by a radiologist as showing no acute intracranial abnormality.
An ED physician assumed care several hours later. He documented that she had signs of meningismus, and he ordered a lumbar puncture to rule out meningitis. During the lumbar puncture several hours later, the woman exhibited seizure symptoms and became unresponsive. She was resuscitated, and the ED physician suspected a subarachnoid hemorrhage. He ordered another head CT. A different radiologist interpreted this CT as positive for a subarachnoid hemorrhage.
The woman was transported via helicopter to a tertiary medical center. The ED physician at the tertiary center diagnosed a large intracranial aneurysm arising from the distal vertebral artery, as well as smaller aneurysms. A neurosurgeon was consulted, and he performed an intracranial embolization. The woman was in the ICU for two weeks without neurological recovery, and her family elected to withdraw all life support measures. She died one week later.
The woman’s family filed a malpractice claim against the first ED physician and hospital, alleging failure to timely diagnose a subarachnoid hemorrhage resulting in her death. The experts who reviewed the care were critical of the first ED physician who did not do or document a thorough neurologic exam nor order any imaging to rule out a serious neurological or vascular condition. The claim was settled with a payment to the family on behalf of the first ED physician.
Who is most at risk for diagnostic error malpractice claims?
In an analysis of our malpractice claims, we identified the most significant drivers of risk, harm, and malpractice loss for healthcare organizations. Diagnostic error allegations are number two in costs and number three in frequency across all care settings. The top responsible specialties and care teams involved in diagnostic error claims include:
- Emergency medicine
- Radiology
- Family medicine
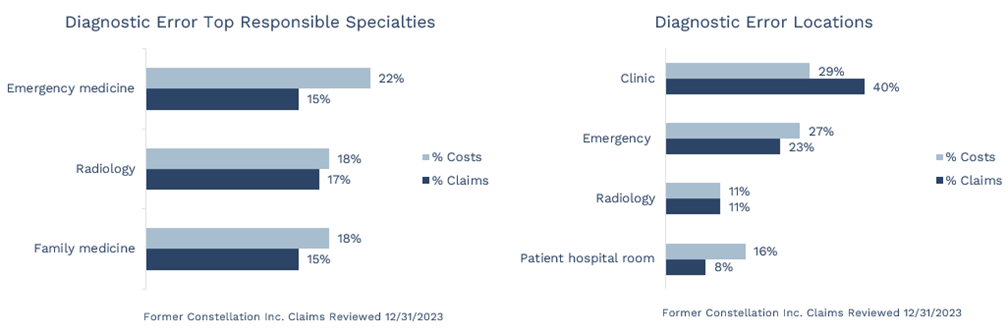
The top locations involved in diagnostic error claims include the clinic, ED, radiology, and patient hospital room. Over half of our diagnostic error claims arise out of care provided in an ambulatory setting—clinics and the ED.
What contributes to diagnostic error harm and malpractice claims?
Knowing the contributing factors involved in diagnostic error harm events helps physicians, care teams, and healthcare organizations develop strategies to reduce risk. As a contributing member of Candello Solutions by CRICO, a national data collaborative of medical professional liability (MPL) insurers and health systems representing over 475,000 MPL claims, we are able to identify the top risk factors contributing to harm events and claims. The top risk factors contributing to diagnostic error claims in the Candello database include:
- Failure to appreciate and reconcile relevant signs/symptoms/test results: 36% of cases
- Failure/delay in ordering a diagnostic test: 33% of cases
- Failure to establish a differential diagnosis list because of a narrow diagnostic focus: 29% of cases
- Misinterpretation of diagnostic studies (images, slides): 26% of cases
- Failure/delay in obtaining a consult/referral: 24% of cases
As this case illustrates, one harm event or claim usually results from multiple contributing factors. In this case, the physician did not appreciate the severity of the patient’s symptoms and did not order a diagnostic test (CT) to rule out a potentially severe neurovascular condition. He also failed to establish a comprehensive differential diagnosis list and instead diagnosed neck strain. There were also criticisms of the initial CT read by the radiologist. The expert reviews indicated that there were some indications of a vascular event present on the CT; however, the radiologist was not named in the malpractice claim filed by the family.
How to mitigate harm and resultant diagnostic error malpractice claims
- Provide clinical decision support tools (e.g., clinical algorithms) to help clinicians develop robust differential diagnosis lists and rule out potentially serious conditions.
- Encourage clinicians to correlate test and image results with the patient’s clinical symptoms.
- Encourage joint strategy discussions between the ordering clinician and the radiologist (e.g., pre-imaging decision-making and post-imaging diagnosis) to improve the diagnostic process.
- Evaluate your clinic or ED test result and referral management systems by mapping these processes and performing a Failure Mode and Effects Analysis (FMEA) to identify and fix vulnerabilities.
- Implement reliable follow-up systems for communicating test results in the clinic and ED (e.g., after discharge, preliminary/final overreads, and incidental image findings).
- Implement clinician feedback regarding diagnostic accuracy (e.g., adverse event reports of missed diagnoses, patient complaints, autopsy reports, radiology overread discrepancies, and peer review).
- Analyze your adverse events using an all cause or root cause analysis tool to identify causal/contributing factors and implement risk strategies to mitigate future adverse events.
How to mitigate harm involved in diagnostic error malpractice claims
Curi and Iowa Healthcare Collaborative are coming together to offer a virtual conference highlighting the impact that harm events from the top drivers of malpractice claims—diagnostic error, surgical treatment, and obstetrical treatment—have for physicians, healthcare providers, organizations, and patients. Attendees will gain valuable insights to understand why these malpractice allegations occur, identify opportunities for improvement, and recognize how early intervention provides a better way forward for all involved after harm.
This conference will take place over three half-days on April 2, 3, and 4, 2024. There is no fee to register, and continuing education credits will be available.
Risk reports
Our risk reports analyze malpractice claim data on a wide range of topics and specialties and share insights clinicians, care teams, clinics, hospitals, and senior living organizations can use to help reduce harm events and malpractice claims. Are you a client? Sign in to MyAccount to access exclusive client versions of our risk reports. The expanded reports share actionable insights and strategies that you can utilize to help reduce harm events and malpractice claims. After you sign in, follow Risk Resources > Tools & Resources > Publications > Risk Reports. You also have access to a host of Bundled Solutions (in Risk Resources) that cover a wide variety of topics—such as Preventing Diagnostic Error—to assist you in your risk mitigation efforts.
Curi’s risk mitigation resources and guidance are offered for educational and informational purposes only. This information is not medical or legal advice, does not replace independent professional judgment, does not constitute an endorsement of any kind, should not be deemed authoritative, and does not establish a standard of care in clinical settings or in courts of law. If you need legal advice, you should consult your independent/corporate counsel. We have found that using risk mitigation efforts can reduce malpractice risk; however, we do not make any guarantees that following these risk recommendations will prevent a complaint, claim, or suit from occurring, or mitigate the outcome(s) associated with any of them.
Share this blog article:
Latest Blog Articles
Five Steps to Reduce Generative AI Risks in Healthcare
AI is already assisting physicians and healthcare organizations in many ways. Learn how its use may impact liability and what strategies can mitigate risk.
Five Steps to Reduce Obstetrical Errors and Malpractice Claims
Learn how to reduce obstetrical harm using evidence-based protocols for managing high-risk situations, joint team fetal monitoring education, and enhanced teamwork.
How to Reduce Surgical Harm and Malpractice Claims
In an analysis of our medical professional liability claims, surgical allegations are #1 in occurrence and #2 in cost. Learn how to reduce surgical malpractice risk.